
LDL Reduction Estimator
Based on research, alternate-day statin dosing typically maintains about 90-95% of the LDL-lowering benefit compared to daily dosing. This calculator helps estimate your LDL levels with alternate-day dosing.
Note: This is for informational purposes only. Always consult your doctor before changing your statin regimen.
For millions of people taking statins to lower cholesterol, the dream isn’t just about hitting a number on a lab report-it’s about being able to climb stairs, walk the dog, or carry groceries without muscle pain. But for 1 in 7 users, daily statins cause muscle aches so bad they quit. That’s where alternate-day statin dosing comes in. It’s not a miracle cure, but for many, it’s the only way to keep taking a life-saving drug without feeling like you’re constantly sore.
Why Alternate-Day Dosing Exists
Statin intolerance isn’t rare. Studies show between 10% and 15% of people who take statins daily develop muscle pain, weakness, or cramps. For some, it’s mild. For others, it’s debilitating. When doctors try switching statins-simvastatin to pravastatin, then to fluvastatin-it often doesn’t help. The problem isn’t the brand. It’s the dose. Daily dosing floods the body with the same drug over and over, and for sensitive people, that’s too much. Enter alternate-day dosing: take your statin every other day instead of every day. This isn’t a new idea. It started in clinics in India and Europe over a decade ago, when doctors noticed patients on atorvastatin or rosuvastatin still had low LDL even after skipping a day. These two statins have long half-lives-up to 30 hours-meaning they stick around in your system long after you swallow the pill. That’s the key. If the drug doesn’t vanish by the next day, you might not need to take it daily.How Much LDL Does It Lower?
The big question: does it work? The short answer is yes-mostly. A 2012 study of 38 people with high cholesterol compared daily 20 mg atorvastatin to every-other-day 20 mg. After 12 weeks, daily dosing lowered LDL by 44.1%. Alternate-day? 42.3%. The difference? Not statistically meaningful. Total cholesterol dropped almost identically too. Other studies with rosuvastatin show similar results: you lose maybe 5-10% of the LDL-lowering power, but you keep 90% of the benefit. This isn’t magic. If your goal is to get LDL below 70 mg/dL (common for people with heart disease), daily dosing still wins. But if you’re trying to avoid muscle pain and your LDL is at 130, alternate-day dosing might get you down to 90-enough to reduce risk without the pain.What About Side Effects?
This is where alternate-day dosing shines. In one study, 23 patients had quit statins because of muscle pain. Every single one of them couldn’t tolerate daily atorvastatin or rosuvastatin. But when they switched to the same drug every other day-plus ezetimibe and colesevelam-87% of them stayed on it. No muscle pain. No quitting. Another study found that switching to alternate-day dosing cut muscle-related side effects by 30% to 50%. That’s huge. For people who’ve given up on statins, this isn’t just a tweak-it’s a lifeline. The reason? Less drug exposure. Your muscles get a break. The liver still gets enough to pull cholesterol out of the blood, but your muscles aren’t being constantly bombarded. It’s like turning down the volume on a speaker instead of turning it off.Which Statins Work Best?
Not all statins are created equal here. Atorvastatin (Lipitor) and rosuvastatin (Crestor) are the only two with solid evidence. Why? Their long half-lives. Atorvastatin lasts 14 to 30 hours. Rosuvastatin sticks around for 19 hours. That’s long enough to cover two days. Simvastatin? Not so much. Its half-life is only 1 to 3 hours. Skip a day, and the drug’s gone. You won’t get much LDL reduction. Pravastatin, fluvastatin, and lovastatin? Same problem. Too short-lived. So if your doctor suggests alternate-day dosing, make sure it’s one of these two. No exceptions.
Cost and Convenience
Here’s a bonus: you save money. A 30-day supply of generic atorvastatin 20 mg costs about $10. If you take it every other day? You’re using half the pills. That’s $5 a month. Over a year? $60 saved. For rosuvastatin? Maybe $100 a year. That’s not life-changing money, but for people on fixed incomes, it helps. Compare that to PCSK9 inhibitors like Repatha or Praluent-$5,000 to $14,000 a year. Or even ezetimibe (Zetia) at $300 a month. Alternate-day statin dosing is cheaper than most alternatives. But there’s a catch. You have to remember to take it every other day. No pill organizer will help if you don’t track it. Some people use phone alarms. Others mark a calendar. A few even use a two-pill system: one color for “take,” one for “skip.”Who Should Try It?
This isn’t for everyone. It’s for a very specific group:- You’ve tried at least two different statins daily and had muscle pain both times.
- Your creatine kinase (CK) levels are normal or only slightly raised (under 10x the upper limit).
- You have a high risk of heart attack or stroke-so you still need strong cholesterol control.
- You’re on atorvastatin or rosuvastatin.
What the Experts Say
The American College of Cardiology doesn’t officially endorse alternate-day dosing. They call it “off-label” and say there’s no proof it reduces heart attacks. That’s true. No large trial has proven it cuts strokes or heart attacks. But here’s the nuance: no one’s proven that ezetimibe or PCSK9 inhibitors reduce heart attacks either in people who can’t take statins. So doctors are using what works. Dr. Robert Rosenson, a top cardiologist, says alternate-day dosing is a “rational approach” for people who can’t take daily statins. The Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC) group calls it “as efficacious as daily dosing” for LDL and triglycerides. In practice, 68% of lipid specialists in the U.S. use it. At academic hospitals? 82%. It’s not fringe. It’s practical.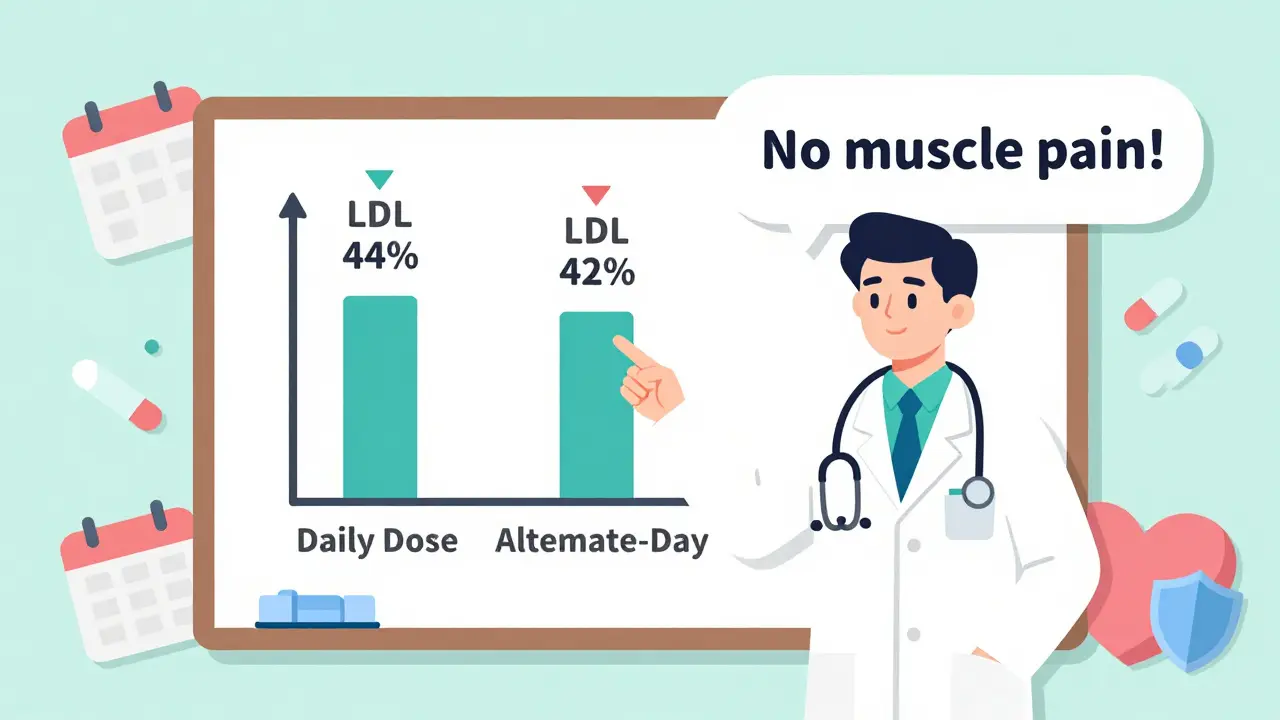
How to Get Started
If you think this might work for you:- Talk to your doctor. Bring up the idea-don’t wait for them to suggest it.
- Get your LDL and CK levels checked before starting.
- Start with 20 mg of atorvastatin or 10 mg of rosuvastatin every other day. Don’t guess the dose.
- Check your LDL again in 4 to 6 weeks. If it’s not down by at least 30%, you may need to add ezetimibe.
- Keep a symptom journal. Note any muscle pain, fatigue, or weakness.
What Doesn’t Work
Some people try skipping days with simvastatin. It doesn’t work. The drug clears too fast. Others try once-a-week dosing. That’s too little. One study found only 27% of people reached their LDL goal on once-weekly rosuvastatin. And never combine this with grapefruit juice. It can spike statin levels-no matter the schedule.The Bottom Line
Alternate-day statin dosing isn’t the future. It’s the present. For people who can’t tolerate daily statins, it’s one of the few tools that actually works. You lose a little LDL-lowering power, but you gain something priceless: the ability to live without constant pain. It’s not perfect. Insurance might not cover it. You’ll have to track your doses. And yes, we still need long-term studies on heart outcomes. But for now? If you’ve been forced to quit statins because of muscle pain, this might be your best option. Talk to your doctor. Try it. You might be surprised at how much better you feel.Can I switch to alternate-day statin dosing on my own?
No. Never change your statin dose without talking to your doctor. Statins are powerful drugs, and even small changes can affect your cholesterol levels or muscle health. Your doctor needs to check your LDL, CK levels, and overall risk before making any adjustment. Self-adjusting could lead to under-treatment or unexpected side effects.
Is alternate-day dosing safe for long-term use?
There’s no long-term data specifically on alternate-day dosing-no studies tracking heart attacks or strokes over 10 years. But the statins used (atorvastatin and rosuvastatin) have decades of safety data with daily use. Since the total weekly dose is similar, experts believe the long-term risks are comparable. Still, regular monitoring of liver enzymes and muscle symptoms is essential.
Does alternate-day dosing work for everyone with statin intolerance?
No. It works best for people with mild to moderate muscle pain (myalgia) and normal or only slightly elevated CK levels. If you have severe muscle damage (rhabdomyolysis) or very high CK, alternate-day dosing isn’t safe. Also, if your LDL is extremely high (over 190 mg/dL), you may still need daily dosing or combination therapy. It’s not a one-size-fits-all solution.
Why don’t more doctors recommend this?
Many doctors aren’t trained on this approach. Medical guidelines focus on daily dosing, and drug labels don’t mention alternate-day use. Plus, insurance systems are built around daily prescriptions. It takes time and experience to get comfortable with off-label strategies. But among lipid specialists-doctors who focus on cholesterol-over two-thirds use it regularly.
Can I combine alternate-day statins with other cholesterol drugs?
Yes, and often you should. Many patients who switch to alternate-day dosing still need help reaching their LDL goal. Adding ezetimibe (Zetia) or a bile acid sequestrant like colesevelam can boost LDL reduction by another 15-20%. These combinations are well-studied and often better tolerated than daily high-dose statins. Your doctor can help you choose the right mix.




