It’s common to see patients on both an H2 blocker and a proton pump inhibitor (PPI) for stomach acid issues. Doctors might think two drugs that reduce acid must work better together. But the science says otherwise. In fact, combining these medications often leads to more side effects, higher costs, and no real benefit for most people.
How H2 Blockers and PPIs Actually Work
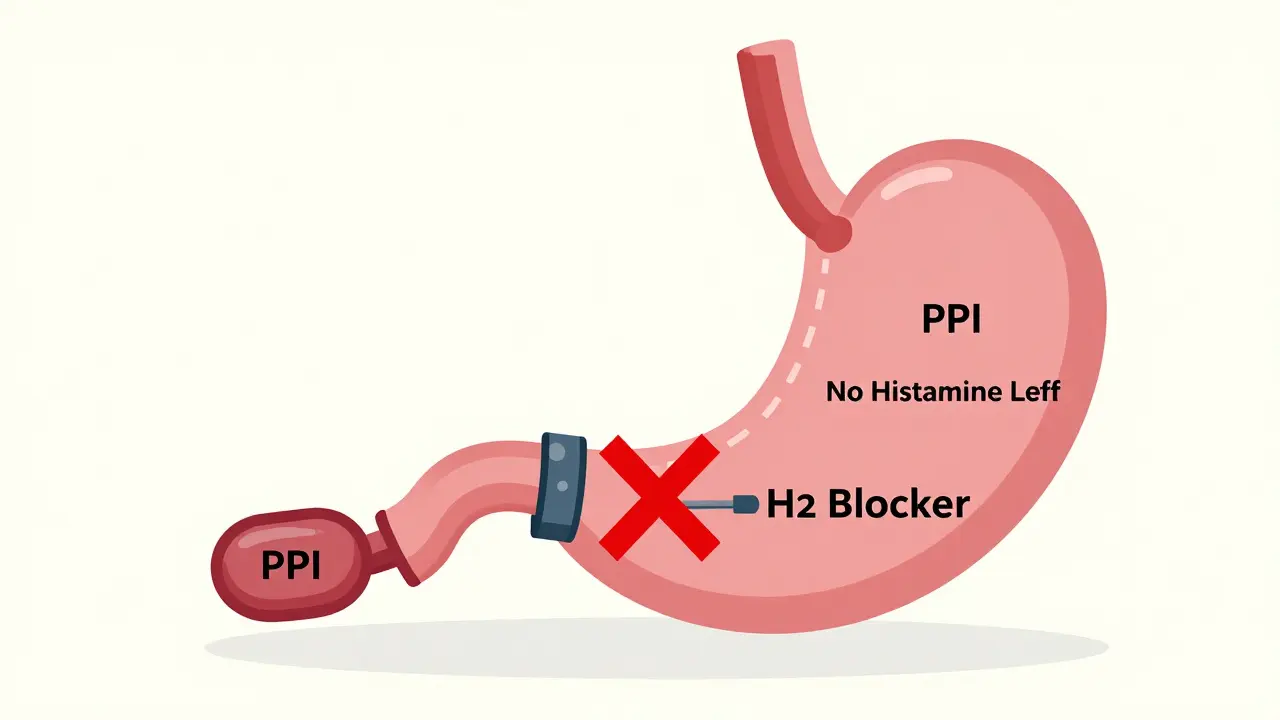
H2 blockers like famotidine (Pepcid) and cimetidine (Tagamet) block histamine from binding to receptors on stomach cells. This cuts acid production by about half. They kick in fast-within an hour-but their effect fades after 6 to 12 hours. That’s why people sometimes take them twice a day.
PPIs like omeprazole (Prilosec) or esomeprazole (Nexium) work differently. They shut down the proton pump-the actual machine that produces acid. This blocks up to 98% of acid, and the effect lasts all day. But they don’t work right away. It takes 2 to 5 days for PPIs to reach full power because the body has to replace the pumps they disable.
Here’s the catch: PPIs suppress acid so completely that there’s almost no histamine left to stimulate the stomach. And that’s a problem for H2 blockers. They need histamine to work. If you’re already on a strong PPI, adding an H2 blocker is like trying to turn off a light with a switch that’s already been unplugged.
The Evidence Says: No Real Benefit
A 2022 study in the Journal of Clinical Gastroenterology looked at patients with GERD who were already on omeprazole. When researchers added ranitidine (an H2 blocker), acid exposure dropped by just 5%-and only at night. No improvement during the day. No better healing of the esophagus. No fewer symptoms.
The American College of Gastroenterology reviewed 12 clinical trials with nearly 3,000 patients. Their 2022 guideline is clear: long-term combination therapy offers no extra benefit for GERD. The same goes for other conditions like ulcers or gastritis. If a PPI alone isn’t working, adding an H2 blocker won’t fix it.
And yet, about 15% to 20% of hospitalized patients still get both drugs. In the U.S., that’s over 1.2 million people a year. The annual cost? Around $1.5 billion. Most of it is wasted.
The Hidden Risks: More Than Just Wasted Money
Combining these drugs isn’t just unnecessary-it’s risky. A landmark 2014 study in JAMA Internal Medicine followed nearly 80,000 ICU patients. Those on PPIs had:
- 30% higher risk of hospital-acquired pneumonia
- 32% higher risk of Clostridium difficile infection
- 22% higher risk of gastrointestinal bleeding
That last one is shocking. You’d think less acid means less bleeding. But PPIs alter the stomach’s natural defenses. They let harmful bacteria grow and weaken the gut lining. H2 blockers don’t do this as much.
Another red flag: kidney damage. A 2021 study in BMC Nephrology tracked over 3,600 patients with chronic kidney disease. Those on PPIs had a 28% higher chance of progressing to end-stage kidney disease compared to those on H2 blockers. The reason? PPIs may trigger a rare but serious condition called acute interstitial nephritis.
On top of that, long-term PPI use is linked to low levels of vitamin B12, magnesium, and calcium. This can lead to fatigue, muscle cramps, and even bone fractures. H2 blockers don’t carry the same risks.
Who Might Still Need Both?
There’s one scenario where combining them might make sense: nocturnal acid breakthrough.
This happens when acid levels spike between midnight and 6 a.m., even while on a PPI. Some patients feel heartburn at night despite taking their PPI in the morning. If this is confirmed by a 24-hour pH monitor showing acid levels above pH 4 for more than 60 minutes during those hours, then adding an H2 blocker at bedtime *might* help.
But even then, it’s temporary. The American College of Gastroenterology says: use the H2 blocker for only 4 to 8 weeks. If symptoms don’t improve, stop it. Don’t keep it going.
And here’s the kicker: many doctors don’t even check for this. A 2022 survey by the ACG found that 31% of patients on both drugs couldn’t explain why they were taking them. Sixty-four percent didn’t know the side effects.
Drug Interactions You Can’t Ignore
Cimetidine, an older H2 blocker, is a known inhibitor of liver enzymes (CYP450). It can raise the levels of other drugs in your blood-like blood thinners, antidepressants, or even some PPIs. This increases the chance of side effects from those medications.
Famotidine doesn’t do this as much. But if you’re on multiple medications, mixing any H2 blocker with a PPI adds complexity. More pills. More chances for something to go wrong.
And don’t forget: PPIs can interfere with how your body absorbs certain drugs. Iron supplements, antifungals, and some antibiotics work less well if taken with a PPI. If you’re on one of these, adding an H2 blocker doesn’t fix the absorption problem-it just adds another layer of confusion.

What Should You Do Instead?
If you’re on both an H2 blocker and a PPI:
- Ask your doctor: Why am I on both?
- Ask if your symptoms are truly controlled on the PPI alone.
- Ask if you’ve ever had pH monitoring to confirm nocturnal breakthrough.
- If not, request a 30-day trial of the PPI alone.
- Track your symptoms during that time. If they stay under control, the H2 blocker can likely be stopped.
For most people, lifestyle changes work better than extra pills:
- Eat smaller meals
- Avoid lying down for 3 hours after eating
- Limit caffeine, alcohol, spicy foods, and chocolate
- Elevate the head of your bed by 6 inches
- Loosen tight clothing around the waist
And if you’ve been on a PPI for over a year? It’s time for a time-out. The VA recommends every 90 days. Ask your doctor to help you taper off slowly-abruptly stopping PPIs can cause rebound acid hypersecretion.
The Bigger Picture: Overprescribing Is a Crisis
Dr. John Inadomi from the University of Washington says 70% of PPI prescriptions are inappropriate. Add an H2 blocker on top, and you’ve created a perfect storm of unnecessary medication.
Regulators are catching on. The FDA has warned about PPIs and bone fractures, kidney injury, and C. diff infections. In 2023, the American Gastroenterological Association added “Don’t prescribe combination therapy with a PPI and H2RA for routine GERD” to its Choosing Wisely list.
And starting in 2024, Medicare will penalize hospitals where more than 15% of patients get this combination without clear medical justification.
The truth? H2 blockers are cheaper, safer, and just as effective for many people. PPIs are powerful-but they’re not always the right tool. And using them together? It’s not better. It’s just more.
9 Comments

Morgan Dodgen
March 11, 2026 AT 08:31 AM
LMAO so the pharma bros are just pushing PPIs because they make 800% margins and H2 blockers are generic as hell? 🤡
Of course the FDA didn’t crack down until Medicare started auditing. This is capitalism 101 - profit over patients. They’ll sell you 3 drugs to fix the side effects of the first one. Next thing you know you’re on anticholinergics for the constipation from the PPIs. 🤯

Philip Mattawashish
March 12, 2026 AT 00:07 AM
You think this is bad? Wait till you find out how many people are on PPIs because their doctor didn’t want to deal with their anxiety-induced GERD. It’s not acid. It’s stress. But nope, let’s just blindfold the patient with a $300/month prescription and call it a day. You’re not treating the root cause-you’re just burying it under chemical fog. Pathetic.

Tom Sanders
March 12, 2026 AT 17:18 PM
I was on both for like 4 years. My doc just shrugged and said ‘it’s fine’. I finally asked why and he said ‘well you’ve been on them so long’. That’s not a reason. That’s just laziness. I dropped the H2 blocker and didn’t even notice a difference. Why did I pay for that?

Jazminn Jones
March 14, 2026 AT 10:45 AM
The clinical evidence presented here is methodologically robust and aligns with the most recent meta-analyses from the Cochrane Collaboration (2023) and the ACG’s Choosing Wisely initiative. The conflation of pharmacodynamic synergy with clinical efficacy remains a pervasive diagnostic fallacy in primary care. One must also account for the confounding variable of polypharmacy-induced iatrogenesis, which disproportionately affects elderly and multimorbid populations. The economic burden is not merely fiscal-it is a systemic erosion of rational therapeutics.

Stephen Rudd
March 16, 2026 AT 04:11 AM
You Americans are ridiculous. In Australia, we don’t even prescribe PPIs for mild reflux. We tell people to stop eating takeaway and go for a walk. You turn every minor discomfort into a pharmaceutical emergency. And now you’re shocked that your healthcare system is bankrupt? Newsflash: you’re not sick. You’re just lazy.

Erica Santos
March 16, 2026 AT 09:00 AM
So let me get this straight. We’ve got a whole generation of people on PPIs because they ate pizza at midnight and thought ‘oh no, I’m dying’? And now we’re pretending the solution is more pills? Classic. The real diagnosis is ‘modern life’ and the cure is ‘get off your couch’. But hey, why fix society when you can fix a pill bottle?

Nicholas Gama
March 18, 2026 AT 08:39 AM
The VA recommends a 90-day taper. But 90% of doctors don’t even know that. This isn’t medicine. It’s autopilot. And the FDA? They’re asleep. They’ll warn about fractures but not the $1.5 billion waste. Because the system doesn’t care if you’re healthy. It cares if you’re profitable.

Mary Beth Brook
March 20, 2026 AT 07:57 AM
This is why America’s healthcare is broken. We treat symptoms like enemies instead of signals. H2 blockers are cheaper, safer, and work fine for 80% of people. But no-let’s push the expensive, branded, patent-protected drug because it’s more profitable. This isn’t science. It’s corporate lobbying with a stethoscope.
Write a comment
Popular Posts


10 Best Alternatives to Bactrim in 2025
Mar, 23 2025


Judith Manzano
March 9, 2026 AT 22:17 PM
I’ve been on PPIs for years and just recently stopped after reading this. My acid reflux got worse at first, but after 3 weeks of lifestyle tweaks-elevated bed, no late dinners, cutting out coffee-it’s been better than it’s been in a decade. Who knew the answer wasn’t more pills?
Also, I didn’t know PPIs could mess with magnesium. My muscle cramps stopped the moment I tapered off. Mind blown.