Drug Reaction Type Checker
What type of reaction did you have?
This tool helps you understand if your reaction to medication was a side effect, true allergy, or intolerance based on the CDC's guidelines.
Check your reaction
Answer these 5 key questions based on your experience:
Your Result
Ever taken a pill and felt off? Maybe your stomach churned, your skin broke out, or you felt dizzy. Then you told your doctor you're "allergic" to it. But here’s the truth: most of the time, you’re not. You’re just experiencing a side effect - and confusing it with a real allergy can cost you more than just time. It can cost you your health.
What’s Really Happening When You Feel Bad After a Pill?
Not all bad reactions to medicine are the same. Three things can go wrong: side effects, allergic reactions, and intolerance. They sound similar, but they’re totally different - and knowing which is which changes everything.Let’s start with side effects. These are predictable, known outcomes of how a drug works in your body. Think of them like the unintended noise from a car engine - it doesn’t mean the car is broken, just that it’s doing its job a little too hard. For example, NSAIDs like ibuprofen cause stomach upset in 25-30% of people. SSRIs like sertraline make 15% of users dizzy. First-gen antihistamines? Around 40% feel sleepy. These aren’t surprises. They’re listed in the drug’s说明书 (package insert). And here’s the good news: they often fade with time. Take metformin with food? That nausea drops by 60%. No need to quit the drug - just adjust how you take it.
True Drug Allergies: When Your Immune System Fights Back
Now, a real drug allergy is something else entirely. This isn’t about the drug’s chemistry. It’s about your immune system mistaking the medicine for an invader. Your body makes antibodies - usually IgE - and goes into attack mode. This can happen within minutes, sometimes seconds. Symptoms? Hives. Swelling of the lips, tongue, or throat. Trouble breathing. A sudden drop in blood pressure. These aren’t just uncomfortable - they can kill.Real allergies are rare. Only 5-10% of all drug reactions are true allergies. Yet, 10% of Americans think they’re allergic to penicillin. The CDC says only 1% actually are. That mismatch is dangerous. People who think they’re allergic to penicillin get stronger, broader antibiotics - which raises their risk of C. diff infection by 30% and MRSA by 50%. One study found that patients with mislabeled penicillin allergies stayed in the hospital 1.2 days longer on average. That’s not just cost - it’s risk.
True allergies come in two flavors. Immediate reactions (Type I) hit fast: within an hour. Think anaphylaxis. Delayed reactions (Type IV) show up days later. DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms) is one. It causes fever, rash, swollen glands, and organ damage. It’s rare but deadly - 10% of cases are fatal. If you’ve ever needed epinephrine, had facial swelling, or struggled to breathe after a drug, you need an allergist. Not your GP. Not a pharmacist. A board-certified allergist.
Intolerance: When Your Body Just Can’t Handle the Dose
Intolerance sits in the middle. It’s not an immune response. But it’s not just a side effect, either. It’s your body being unusually sensitive. You get a normal dose - and your system reacts like it got triple that amount.Take aspirin. Most people take it fine. But 7% of adults with asthma develop severe nasal polyps and wheezing after taking it. That’s not an allergy. It’s intolerance. The same goes for codeine. Some people have a gene variation (CYP2D6 duplication) that turns codeine into morphine too fast. They get violently sick from a normal dose. They’re not allergic - they’re just metabolizing it differently. The key? They might still be able to take other drugs in the same class. A person with aspirin intolerance can often take celecoxib (a COX-2 inhibitor) without issue. That’s not possible with a true allergy.
How to Tell Them Apart: A Simple Guide
Here’s how to sort it out in real life:- Side effect? You feel nauseous, dizzy, or tired. It started within hours of taking the drug. It’s dose-related - take less, and it gets better. You’ve had it before. It didn’t get worse with the next dose. You didn’t need emergency care. This is likely a side effect.
- Allergy? You broke out in hives. Your face swelled. You couldn’t breathe. You passed out. You needed epinephrine. This happened within minutes to an hour. You’ve had it before - and it got worse each time. This is a true allergy. You need to avoid the drug forever - and carry an EpiPen.
- Intolerance? You got a normal dose. You had a severe reaction - but not hives or swelling. Maybe you got asthma symptoms after NSAIDs. Or violent vomiting from codeine. You’ve tried the same drug twice and had the same issue. But other drugs in the class? Fine. This is intolerance. It’s not an allergy, but you still need to avoid that class.
Don’t rely on memory. Don’t guess. Write down what happened: the drug name, the dose, the timing, the symptoms, how long it lasted, and whether you needed medical help. That’s your best tool.
Why This Matters More Than You Think
Mislabeling a side effect as an allergy isn’t harmless. It’s a public health problem. In the U.S., penicillin allergy mislabeling alone costs $1.2 billion a year. Why? Because doctors avoid the best, cheapest, safest antibiotic - and reach for something broader, costlier, and more likely to cause resistance. One patient avoided all antibiotics for 15 years because they thought they were allergic after one bout of nausea. They got tested. Turns out, they weren’t. They’ve taken amoxicillin eight times since - safely.And it’s getting worse. Electronic health records still let doctors just type "allergy" without details. But new systems are changing that. Epic and other platforms now prompt: "Was this a rash? Breathing trouble? Did you need epinephrine?" They’re forcing specificity. Because vague labels kill.
What Should You Do?
If you’ve ever said, "I’m allergic to..." about a drug - pause. Ask yourself:- Did I have hives, swelling, or trouble breathing?
- Did it happen within an hour?
- Did I need emergency treatment?
- Did it happen more than once?
If you answered no to all of those - you probably aren’t allergic. You might have a side effect. Or an intolerance. Either way, you can likely take the drug safely - with the right guidance.
Get tested. Especially if it’s penicillin. Skin tests are quick. Oral challenges are safe under supervision. The new point-of-care penicillin test - expected to be widely available by 2026 - gives results in 15 minutes. That’s faster than your coffee break.
Don’t carry a label you don’t need. Your next doctor shouldn’t have to guess. You deserve the right medicine - not the one they’re forced to use because you thought nausea meant allergy.
Can a side effect turn into an allergy?
No. Side effects and allergies are caused by completely different mechanisms. A side effect is your body reacting to the drug’s chemistry. An allergy is your immune system attacking it. One doesn’t become the other. But if you keep taking a drug and develop new symptoms like hives or swelling - that’s a new reaction. It could be an allergy starting up. That’s rare, but it happens. If symptoms change, get evaluated.
I had a rash after taking amoxicillin. Does that mean I’m allergic?
Not necessarily. A non-itchy, flat rash that appears days after starting amoxicillin - especially in kids - is often a viral rash, not a drug allergy. True allergic rashes are usually itchy, raised (hives), and show up within hours. If the rash was widespread, itchy, or came with swelling or breathing issues, see an allergist. If it was mild and faded on its own, you might still be able to take penicillin. Testing clears up 90% of these cases.
Can I outgrow a drug allergy?
Yes - especially with penicillin. Studies show that 80% of people who had a true penicillin allergy 10 years ago lose their sensitivity over time. That’s why testing is so important. If you were told you were allergic as a child, get retested as an adult. You might be able to use the safest, most effective antibiotic - instead of a risky, expensive alternative.
What if I’m not sure what happened? Should I still avoid the drug?
Don’t avoid it blindly. If you’re unsure - and you didn’t have life-threatening symptoms - talk to an allergist. Self-avoidance leads to worse outcomes. The CDC recommends testing for anyone with a history of penicillin allergy, especially before surgery or hospitalization. Avoiding a drug without knowing why is riskier than using it after proper testing.
Are there tests for drug intolerance?
Not always. Intolerance is often diagnosed by process of elimination. If you react badly to all NSAIDs but not to a COX-2 inhibitor like celecoxib, that’s a clue. For some drugs, genetic tests exist - like HLA-B*57:01 for abacavir (an HIV drug). But for most, it’s about careful re-challenge under medical supervision. If you’ve had a severe reaction, don’t try this yourself. Always work with a specialist.
Popular Posts
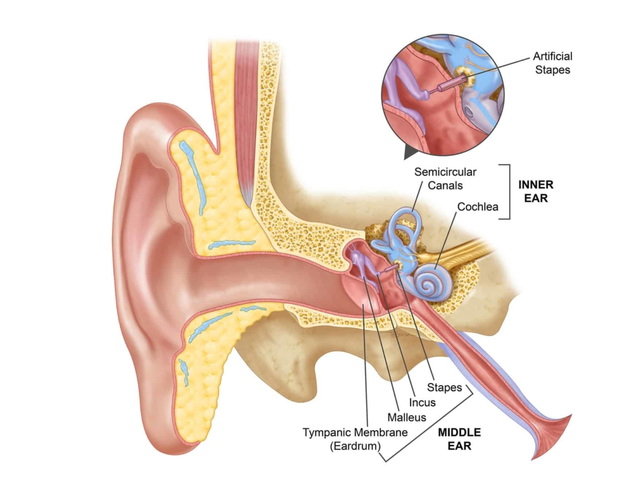
Common Misconceptions About Ear Canal Infections
Apr, 30 2023