
When you walk into a doctor’s office for a routine checkup, you expect your provider to know exactly what medication you need. But what if that decision isn’t made by one person alone? In today’s healthcare system, generic prescribing isn’t just a cost-saving tactic-it’s the result of a coordinated team effort. And the people making those decisions aren’t just doctors anymore.
Who’s Really Deciding Your Medications?
For years, prescribing was seen as a solo act. The doctor diagnosed, wrote the script, and that was it. But research from the National Academy of Medicine shows that’s no longer enough. When patients have three or more chronic conditions-like diabetes, high blood pressure, and high cholesterol-they’re often taking five or more medications. That’s a lot to track. And a lot to get wrong. That’s where team-based care comes in. It’s not a buzzword. It’s a structured system where pharmacists, nurses, care coordinators, and physicians work together-each with defined roles-to make sure medications are safe, effective, and affordable. And generic drugs? They’re a big part of that. Pharmacists aren’t just handing out pills anymore. They’re reviewing every medication a patient takes, spotting interactions, checking for duplicates, and recommending cheaper, equally effective generic alternatives. A 2022 study from the American Pharmacists Association found that when pharmacists are embedded in care teams, medication errors drop by 67%. That’s not luck. That’s process.How the Team Works: Roles That Actually Matter
Think of a team-based care model like a well-rehearsed orchestra. Each member plays a different instrument, but they all follow the same score.- Physicians handle complex diagnoses and make final decisions on treatment plans. But they don’t do all the medication legwork anymore.
- Pharmacists lead medication reviews. They check for drug interactions, assess adherence, and recommend generic switches based on clinical guidelines-not just cost.
- Nurses and medical assistants monitor chronic conditions, track blood pressure or blood sugar trends, and flag when a medication isn’t working.
- Care coordinators make sure everyone’s on the same page. They update electronic records, schedule follow-ups, and connect patients with social services if they can’t afford meds.
Why Generic Prescribing Works Better in Teams
Generic drugs are just as safe and effective as brand-name versions. The FDA requires them to have the same active ingredients, dosage, and performance. But many patients never hear that from their doctor. They’re scared of “cheap” meds. Or they don’t know generics exist. That’s where pharmacists step in. They’re trained to explain the science behind generics. They know which ones have been used for decades with proven results. And they’re the ones who actually talk to patients about cost. In a team setting, a pharmacist can flag that a patient is on a $300/month brand-name statin when a $12 generic works just as well. The nurse confirms the patient’s cholesterol levels are stable. The care coordinator checks if they qualify for a discount program. The doctor approves the switch. All in one visit. Studies show this approach cuts annual drug costs by $1,200 to $1,800 per patient. It also reduces hospital readmissions by 17.3%. That’s because when patients understand why they’re switching to a generic-and feel supported in the process-they’re more likely to take it.
The Tech That Makes It All Work
None of this happens without good systems. A team can’t coordinate if everyone’s using different notes or missing updates. Electronic health records (EHRs) need to be set up for team-based workflows. That means:- Shared medication lists visible to all providers
- Alerts when a pharmacist recommends a generic change
- Automated reminders for medication reviews
- Secure messaging between team members
Challenges No One Talks About
It’s not all smooth sailing. Some doctors still see team-based care as “taking away their authority.” But that’s a myth. The goal isn’t to replace physicians-it’s to free them up. Before team-based care, doctors spent hours on phone calls with pharmacies, chasing down refill authorizations, or explaining why a patient’s meds weren’t working. Now, pharmacists handle 80% of those tasks. One physician on Doximity said it took him 2.5 extra hours a week just to get the system running. But after six months? He got that time back-and then some. Another issue? Communication gaps. The Commonwealth Fund found that 12% of patients in team-based models reported confusion when prescriptions changed without clear explanation. That’s not the team’s fault-it’s a workflow problem. If a pharmacist switches a med and doesn’t document it clearly, the next provider doesn’t know. That’s why daily 15-minute huddles matter. So do standardized templates for documenting changes. The CDC has a free CPA (Collaborative Practice Agreement) template that many clinics now use. It spells out exactly who can do what-and who signs off.
Who Benefits the Most?
This model shines in chronic disease management. If you have diabetes, heart failure, COPD, or high blood pressure, team-based care isn’t optional-it’s life-changing. For example, the CDC’s 2023 Cardiovascular Health Guide recommends pharmacist-led teams for managing hypertension. Why? Because controlling blood pressure often means trying three or four different meds. A pharmacist can help pick the right combo, avoid side effects, and switch to generics that cost a fraction of the price. Patients on Medicare Part D are already eligible. As of 2023, 12.3 million people get free medication reviews through this program. Starting in 2023, eligibility expanded: you only need four medications (down from five) to qualify. That adds over 4 million more people to the program. Even rural patients benefit now. Telepharmacy services have grown by 214% since 2020. A patient in rural Montana can video-call a pharmacist in a city clinic, get a full med review, and have their local pharmacy fill the new prescription-all without driving two hours.What’s Next? AI and the Future of Prescribing
The next frontier? Artificial intelligence. At Mayo Clinic, pilots are using AI tools to scan patient records and suggest generic alternatives that match clinical guidelines. The system doesn’t make the call-it just flags options. The pharmacist reviews it. The doctor approves. The patient gets the info. In early tests, AI increased appropriate generic use by 22% and cut adverse drug events by 9.3%. That’s huge. But it’s not replacing humans. It’s making them faster and smarter. Healthcare leaders are betting big on this. In Q2 2023, 92% of executives said they plan to expand team-based medication services. The only question? Will insurance pay for it? Right now, only 41% of team-based medication services are fully reimbursed. That’s a problem. But with CMS pushing for mandatory medication management in Medicare Advantage plans, that’s changing.Real Talk: Is This Right for You?
If you’re on multiple meds, especially for chronic conditions, ask your provider: “Is there a team that reviews my medications?” If you’re a provider: Start small. Add one pharmacist to your workflow. Use free CDC templates. Train your staff. Track your results. The data doesn’t lie. Team-based care reduces errors, cuts costs, and improves outcomes. And when it comes to generic prescribing, it’s not just about saving money-it’s about making sure the right drug gets to the right person, at the right time, without confusion or fear. This isn’t the future of care. It’s already here.8 Comments

Andrea Beilstein
December 10, 2025 AT 21:13 PM
The system is broken not because we lack teams but because we lack trust in each other. The doctor thinks the pharmacist is overstepping the pharmacist thinks the doctor is out of touch the nurse is drowning in paperwork and the patient just wants to feel heard. Maybe the real generic here is compassion

Simran Chettiar
December 11, 2025 AT 08:23 AM
In the Indian context, we have been practicing team-based medication management for decades through Ayurvedic and Unani systems where the pharmacist, the herbalist, and the diet advisor all collaborate. The Western model is just catching up. The FDA’s standards are good, but the cultural acceptance of generics is still low. People here believe expensive equals effective. This mindset needs to change through education, not just policy.

Anna Roh
December 11, 2025 AT 11:28 AM
I’ve had my meds switched to generics twice. First time I got the wrong one. Second time I got the same one but it made me dizzy. So yeah, nice theory. In practice? Still a crapshoot.

Jennifer Blandford
December 13, 2025 AT 02:37 AM
THIS. IS. EVERYTHING. 🙌 I’ve been on 7 meds for years and my pharmacist actually sat with me for 45 minutes and said ‘hey, this $200 pill? You can get the same thing for $4.’ I cried. Not because I was sad-because someone finally cared enough to explain. Team-based care isn’t just efficient-it’s human. And we need more of it.

Christian Landry
December 13, 2025 AT 09:04 AM
lol i used to think pharmacists just handed out pills til my buddy got his blood pressure meds switched and his copay dropped from $180 to $12. now he texts me pics of his receipt like its a trophy 🤣 honestly tho the VA system is wild how it auto-suggests generics. my doc just clicks approve and boom. done.

Sarah Gray
December 15, 2025 AT 01:42 AM
The claim that generic prescribing improves outcomes is statistically misleading. Studies cherry-pick patients with stable conditions. In real-world practice, generic switches increase non-adherence due to perceived inferiority. The 67% error reduction? Likely inflated by automated alerts, not clinical judgment. This is techno-bureaucratic fetishism dressed as innovation.

Tejas Bubane
December 15, 2025 AT 03:08 AM
Team-based care? More like team-based bureaucracy. Doctors are being turned into rubber stamps. Pharmacists are now the real prescribers and no one’s talking about liability when something goes wrong. And don’t get me started on AI-next thing you know, an algorithm will decide if your depression is ‘cost-effective’ to treat. This isn’t progress. It’s rationing with a smile.
Write a comment
Popular Posts

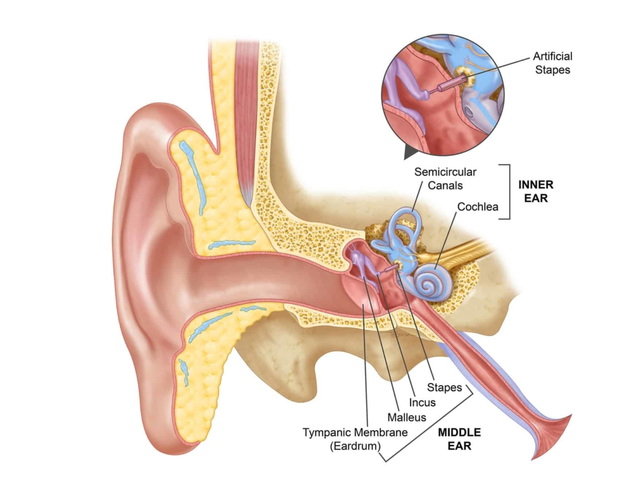
Common Misconceptions About Ear Canal Infections
Apr, 30 2023

Angela R. Cartes
December 10, 2025 AT 05:34 AM
Ugh, another ‘team-based care’ fairy tale. 🙄 So now pharmacists are the new gods of prescriptions? Next they’ll be doing the physicals too. I’ve seen these ‘cost-saving’ swaps-half the time the generic makes me feel like a zombie. Not all generics are created equal, folks.